
Feline lungworm and heartworm
Lungworm and heartworm are an underestimated but potentially serious threat for many cats, as this article reveals.
Issue number 32.2 Other Scientific
Published 30/11/2022
Also available in Français , Deutsch , Italiano and Español
Chylothorax is a differential for any cat with pleural effusion; here Elizabeth Rozanski describes her preferred approach to such cases.

Chylothorax is most common in middle-aged cats, and can be an exceedingly frustrating disease to treat, for both owners and clinicians.
A chylothorax effusion typically has a milky appearance, but where there has been prolonged anorexia, the fluid may be clear or only slightly cloudy.
Surgical ligation of the thoracic duct is a common therapeutic option, although it requires meticulous preparation and attention to detail, and failure is not uncommon.
Although feline chylothorax can be a frustrating condition to treat, careful attention to the diagnostic testing process and a strategic choice in therapeutics can achieve a successful outcome.
Chylothorax develops where there is accumulation of chyle within the thorax 1,2,3,4. Chyle is the lymphocyte-rich fluid that drains with chylomicrons following digestion in the intestines. Chyle is usually shunted back into the vasculature and promotes a healthy immune system and prevents malnutrition, but chylous effusion develops when the normal thoracic duct drainage is impaired. Cats that are affected by chylothorax tend to be middle-aged, with the first clinical sign usually being tachypnea or restrictive breathing. Chylothorax can be an exceedingly frustrating disease for both owners and clinicians, and the condition is rare enough that there are limited studies, so it is difficult to accurately advise on the best approach for treatment. Owners of cats with chylothorax should therefore be counseled at the outset that the disease can be very challenging.
In order to better understand chylothorax and why it might develop, it is helpful to review the relevant anatomy and physiology. In brief, the lymphatics drain the intestines of lipids (chylomicrons) and plasma proteins 1,5. These lymphatics coalesce at the cisterna chyli and are joined by lymphatics from the abdominal cavity and pelvic limbs; these then form the thoracic duct which crosses the diaphragm to join the circulatory system at the junction of the caudal jugular vein and cranial vena cava. The junction has a one-way valve, so that while chyle can join the venous circulation, blood cannot flow in a retrograde direction. In order for chylous effusion to develop there needs to be an obstruction to the drainage, trauma to the thoracic duct, or malformation or dilatation of the duct system (lymphangiectasia) 1,2,3,4.
When a pleural effusion is identified, either based upon physical examination, radiography or ultrasonography, thoracocentesis should be performed in order to remove as much fluid as possible; this is both diagnostic and therapeutic (Figure 1). An aliquot of fluid should be saved for analysis from all thoracocentesis cases if the underlying cause is not known, or if the fluid has changed in appearance from previous samples, or if the clinical condition of the cat has altered.

Figure 1. Thoracocentesis is mostly commonly performed with the cat gently restrained in sternal recumbency. Sedation (e.g., butorphanol 0.1-0.4 mg/kg IV or IM) may be necessary. A butterfly catheter (19-21G), over the needle catheter (20-22G), or 1.5 inch/4.5 cm 22G needle may be used. In large or overweight cats, care should be taken to ensure the needle is long enough to reach the thoracic cavity. The centesis site is usually the 7-9th intercostal space at approximately the level of the costochondral junction.
© Elizabeth Rozanski
Diagnosis of chylothorax is made by fluid analysis, with the pleural effusion containing small lymphocytes and markedly increased triglycerides in relation to cholesterol 1. Most commonly, the effusion has a milky appearance (Figure 2), but in cases of prolonged anorexia, it may be clear or only slightly cloudy. Another type of fluid, termed pseudochylous effusion, is rarely seen, and is represented by fluid that appears cloudy but has a low triglyceride level and often with high cholesterol content. Following the identification of chylous effusion, a search for the underlying cause should be pursued; most cases are likely idiopathic, but in some cases a specific etiology is found, which may allow targeted treatment 1.

Figure 2. Chylous effusion typically appears milky – similar to propofol in appearance – with a high triglyceride concentration, although there may be a pinkish tinge associated with trauma from thoracocentesis. Cytologically, there is an abundance of small lymphocytes.
© Elizabeth Rozanski
Elizabeth Rozanski
Following identification of chylothorax, and after confirmation of the owner’s wishes to proceed with therapy, the following tests can be considered and performed as necessary.
While trauma has historically been considered a potential cause of chylothorax, current evidence suggests that a traumatized thoracic duct (e.g., where there has been inadvertent damage during surgery) will usually heal within 1-2 weeks. However, if there is the possibility of a traumatic event (e.g., a fall or road-traffic accident) this may be meaningful, and certainly any recent thoracic surgical therapy should be considered a potential contributor 6. Other significant historical questions include prior knowledge of cardiac disease, feline leukemia status, and living in an endemic heartworm area. On examination particular attention should be paid for evidence or presence of a heart murmur or gallop rhythm, thyroid enlargement, decreased chest wall compliance (e.g., with a suspected mediastinal mass), muscle mass loss, ascites or other evidence of chronic disease. Long-standing (>3 months) chylous effusion can result in malnutrition, including a lack of fat-soluble vitamins 7. Transvenous pacemaker placement in cats has historically been associated with chylothorax, and therefore these pacemakers are now rarely (if ever) used in this species. In dogs, dialysis catheters, transvenous pacemakers or long-standing central lines have also been linked to the development of chylous effusion due to thrombosis or obstruction of the cranial vena cava.
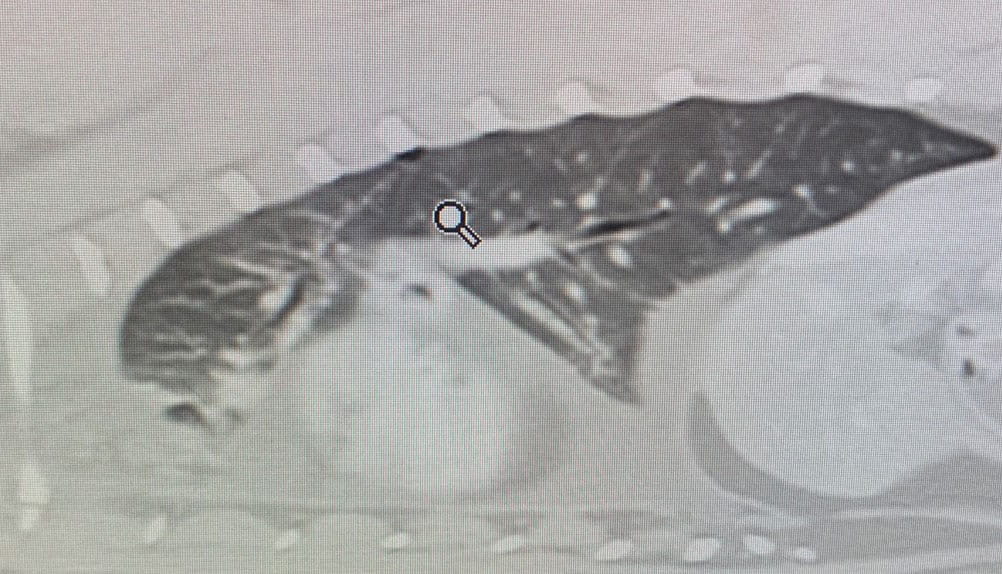
After identification and removal of a pleural effusion, radiographs are useful to evaluate for the presence or absence of restrictive pleuritis, and to check for evidence of cardiomegaly or intrathoracic masses; radiographs prior to the removal of pleural effusion are rarely helpful in determining an etiology. Restrictive pleural effusion may be suspected when the lung fields appear rounded on radiography (Figure 3); this is important to identify if present, as affected cats are at particular risk of developing pneumothorax after thoracocentesis. There are two possible causes for this:

Figure 3. A lateral thoracic radiograph from a cat with restrictive pleuritis; note the rounded lung lobes (solid blue line) and the pneumothorax ex vacuo (dotted blue line) following removal of the chylous effusion.
© Elizabeth Rozanski
Echocardiography is extremely useful for identification and confirmation of cardiac disease as the underlying cause of chylous effusion. Right-sided or biventricular heart failure has been associated with the development of chylous effusion due to increased venous pressure that prevents the thoracic duct from draining into the venous circulation 4. Treating the underlying cardiac disease will help reduce the chylous effusion. Echocardiography can also be used to evaluate for evidence of heartworm disease, along with masses or thrombi in the cranial vena cava. There is one report of a cat with aortic endocarditis identified on echocardiography which was associated with chylous effusion 9.
Fluid analysis is required for the diagnosis of chylothorax, but in addition routine laboratory tests, including a complete blood count, biochemistry profile and urinalysis, are indicated, as for any sick cat. Tests for heartworm antigen and antibody, and retrovirus (FELV and FIV) infection should also be considered, and in patients greater than 5 years of age a thyroid panel is recommended 10. A NT-proBNP test, (which can be performed on pleural effusion) is useful to evaluate for cardiac disease if echocardiography is not available.
Thoracic radiographs after thoracocentesis are useful for documenting any signs of restrictive pleuritis and for evidence of any neoplasia, and if there is suspicion of a mediastinal mass thoracic ultrasound may also be pursued 11. However, a computed tomography (CT) scan, ideally with lymphangiogram, is considered the best imaging modality to look for abnormal thoracic ducts (lymphangectasia) or masses (Figure 4). A CT lymphangiogram may be performed following injection of contrast material into the metatarsal pad 12. Thrombi or masses in the cranial vena cava can also be visualized on CT.
 |
| a |
 |
| b |
© Elizabeth Rozanski
In cases of chylothorax without an apparent underlying cause, thoracic duct ligation (TDL), either alone or in combination with other procedures, is commonly recommended 1,2,13,14. The goal of ligating the thoracic duct is to prevent chyle from entering the chest. Abdominal lymphaticovenous anastomoses subsequently form, allowing the chyle to re-enter the circulation via this route 14. TDL surgery is obviously not beneficial if there is concurrent abdominal chylous effusion, and the procedure requires careful attention to detail; unlike many surgical procedures the success rate is poor, hovering between 50-75%, with the higher percentage anecdotally associated with more meticulous and experienced surgeons. Typically, a lateral thoracotomy is performed, although occasionally a thorascopic approach can be pursued, recognizing the limitations in visualization given the small size of the feline species 15. While there is typically one large duct, it is not uncommon to have multiple smaller ducts that can grow or expand after the first is ligated, and these additional ducts represent one reason for the apparently high surgical failure rate. Visualization of the ducts may be enhanced by feeding a heavy fat (e.g., cream or a kitten food) meal 2-3 hours before surgery, or via the use of new methylene blue dye. Intra-operative lymphangiograms may also provide real time assessment of results.
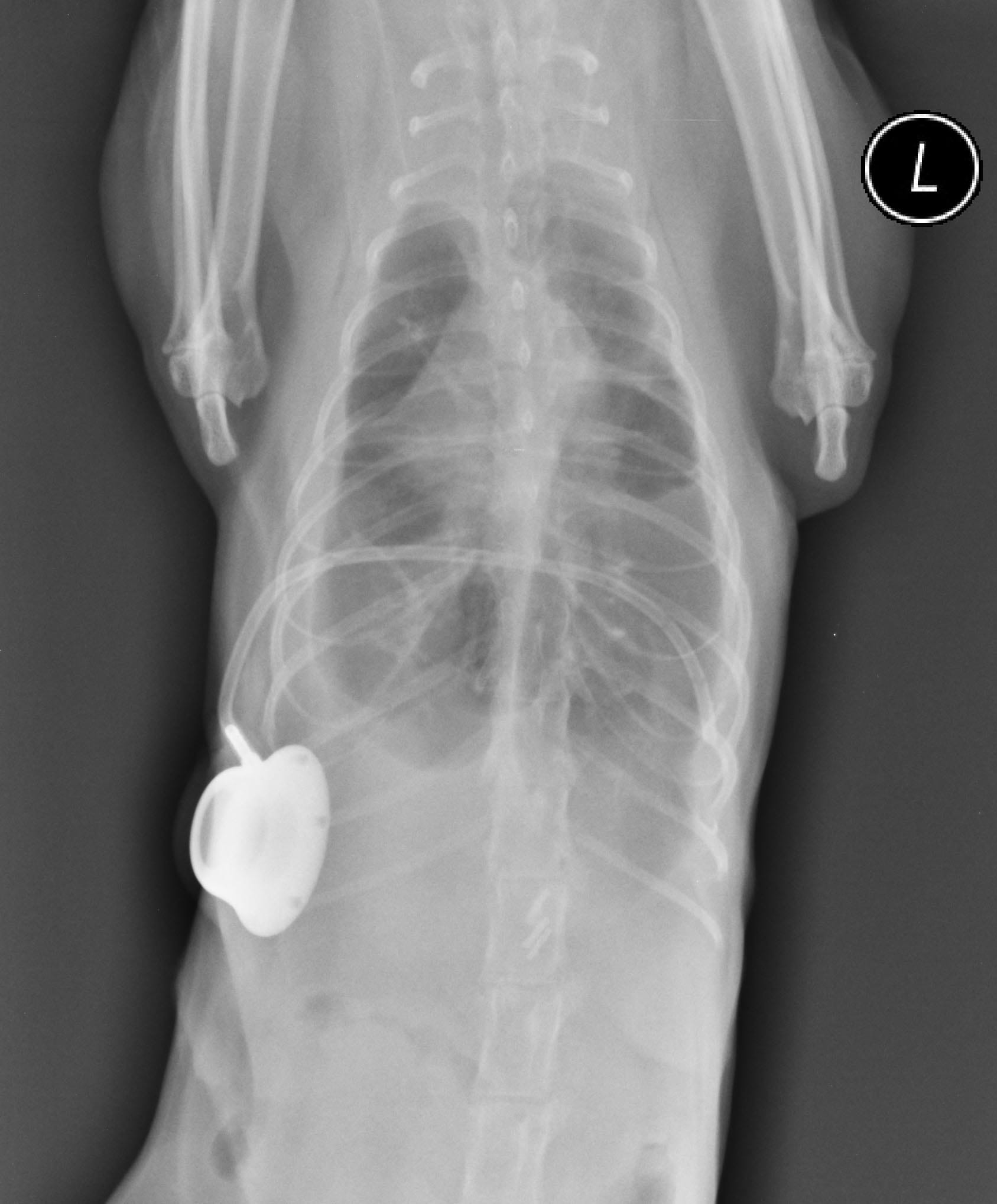
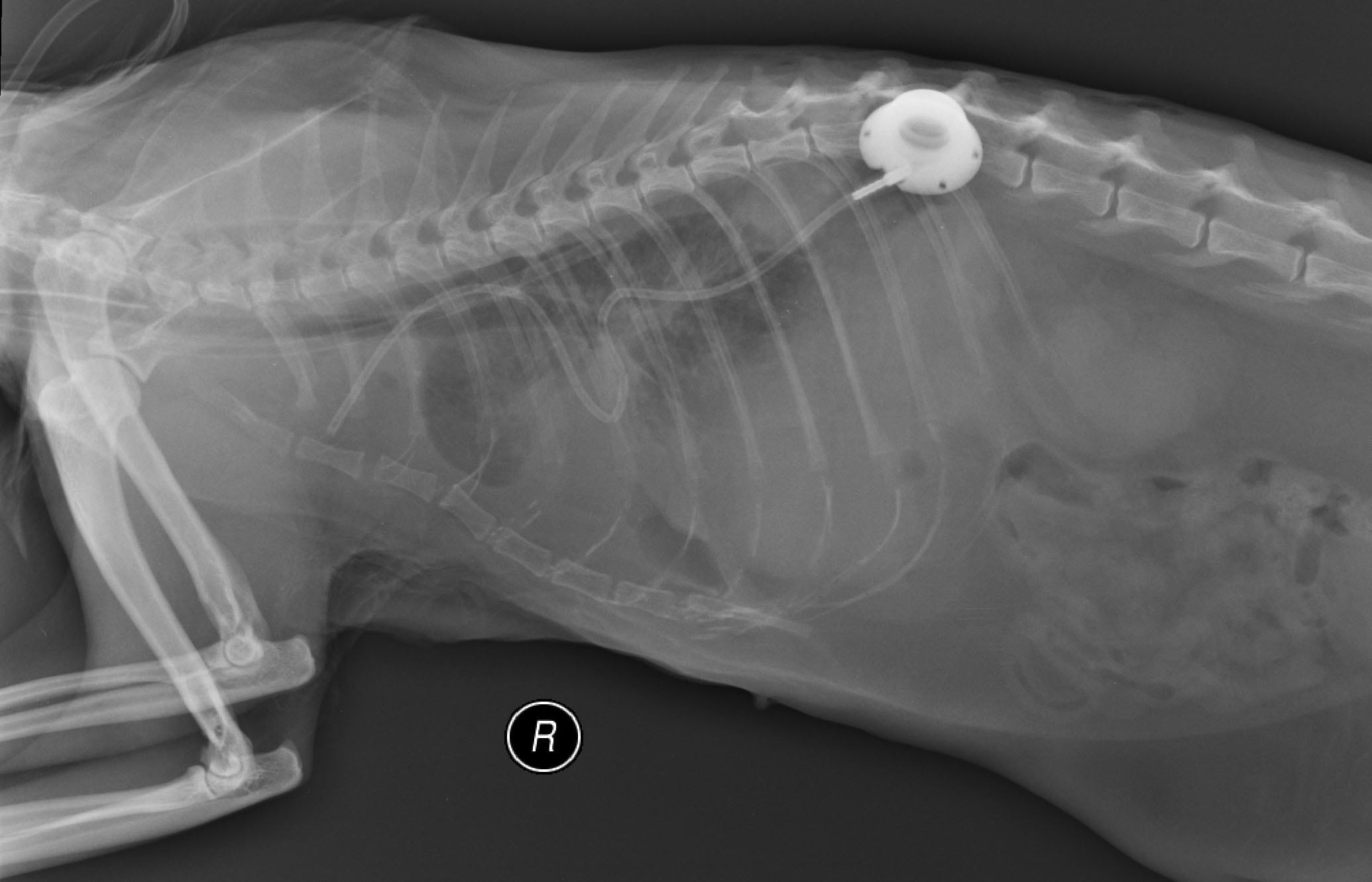
TDL is commonly combined with subphrenic pericardiectomy; one small study in cats found no benefit to also including cisterna chyli ablation 2. A pleuro-port is commonly placed at the time of surgery, and this can permit thoracic drainage at home if the owner and cat are amenable (Figure 5). However, ports can become clogged or non-functional, and pyothorax is also possible if careful adherence to asepsis is not followed.
In dogs, interventional therapy by way of gluing the thoracic duct has reported; the goal of this procedure is to effectively occlude all the branches of the duct 16. To my knowledge, this has not been attempted in cats, but might be worth exploring.
 |
| a |
 |
| b |
Figure 5. A pleuro-port, as seen on these post-surgery radiographs, can be placed to permit thoracocentesis at home, or to reduce the risk of trauma from repeat needle insertions required to drain recurrent effusion.
© Elizabeth Rozanski
Medical therapy is only indicated if any underlying disease such as congestive heart failure (CHF) is detected. Older reports suggested the potential utility of the nutraceutical rutin, but there is no current evidence that it is helpful. Similarly, medium-chain triglycerides (MCT) were previously advocated, since it was thought MCT were absorbed via the lymphatics. This approach has not been shown to be beneficial either, and is no longer recommended. A low-fat diet, if tolerated, may be considered, although there is really no evidence to suggest that this is helpful.
In human medicine, octreotide has been described as a non-surgical therapy for chylothorax, with moderate success in infants 17. The idea is that octreotide decreases the secretions in the gastrointestinal tract, although the exact mechanism of action is unknown. There have been no formal evaluations of this drug for feline chylothorax, but one abstract from almost 20 years ago described some success in a small group of cats 18.
The presence of chyle is very irritating to the pleural surfaces and – as noted above – a thick layer of fibrotic scar tissue can form on the surface of the visceral pleura. This change is particularly worrisome because it is associated with the development of two potential complications, namely restrictive pleuritis, and iatrogenic pneumothorax following thoracocentesis. Restrictive pleuritis is commonly associated with chronic effusion, and results in small lungs that have difficulty with gas exchange. Severe restrictive pleuritis has been historically considered a death sentence, although one recent case report describes successful surgical management 19. Other complications of chylothorax include malnutrition and loss of fat-soluble vitamins (e.g., vitamin K) associated with the loss of chyle, so if recurrent thoracocentesis is performed frequently (i.e., weekly/biweekly), supplementation with fat soluble vitamins could be considered. Immunodeficiency is also a possible risk where there has been a recurrent loss of large volumes of chyle via thoracocentesis 7. However, the most common concern is failure to resolve the effusion, and the subsequent need for ongoing veterinary visits, which can be both expensive for the family and stressful on the cat.
Chylothorax is a frustrating condition for the clinician, but with careful attention to diagnostic testing and strategic choice of therapeutics it can be a rewarding condition to treat. However, clinical trials for evidence-based decision-making on the surgical and non-surgical intervention options for the management of idiopathic effusion are desperately needed. When a cat is identified with chylous effusion, thoracocentesis followed by a prompt search for an underlying cause and early surgical intervention is likely associated with the best prognosis.
Reeves LA, Anderson KM, Luther JK, et al. Treatment of idiopathic chylothorax in dogs and cats: a systematic review. Vet. Surg. 2020;49(1):70-79.
Stockdale SL, Gazzola KM, Strouse JB, et al. Comparison of thoracic duct ligation plus subphrenic pericardiectomy with or without cisterna chyli ablation for treatment of idiopathic chylothorax in cats. J. Am. Vet. Med. Assoc. 2018;252(8):976-981.
Fossum TW, Evering WN, Miller MW, et al. Severe bilateral fibrosing pleuritis associated with chronic chylothorax in five cats and two dogs. J. Am. Vet. Med. Assoc. 1992;201(2):317-324.
Fossum TW, Miller MW, Rogers KS, et al. Chylothorax associated with right-sided heart failure in five cats. J. Am. Vet. Med. Assoc. 1994;204(1):84-89.
Alexander JS, Ganta VC, Jordan PA, et al. Gastrointestinal lymphatics in health and disease. Pathophysiology 2010;17(4):315-335.
Greenberg MJ, Weisse CW. Spontaneous resolution of iatrogenic chylothorax in a cat. J. Am. Vet. Med. Assoc. 2005;226(10):1667-1670, 1659.
Hoskote AU, Ramaiah RN, Cale CM, et al. Role of immunoglobulin supplementation for secondary immunodeficiency associated with chylothorax after pediatric cardiothoracic surgery. Pediatr. Crit. Care Med. 2012;13(5):535-541.
Khan H, Fernandez-Perez ER, Caples SM. Post-thoracentesis trapped lung. J. Postgrad. Med. 2007;53(2):119-120.
Dixon-Jimenez A, Margiocco ML. Infectious endocarditis and chylothorax in a cat. J. Am. Anim. Hosp. Assoc. 2011;47(6):e121-126.
Hayes G. Chylothorax and fibrosing pleuritis secondary to thyrotoxic cardiomyopathy. J. Small Anim. Pract. 2005;46(4):203-205.
Meadows RL, MacWilliams PS, Dzata G, et al. Chylothorax associated with cryptococcal mediastinal granuloma in a cat. Vet. Clin. Pathol. 1993;22(4):109-116.
Chiang C, Chen KS, Chiu HC, et al. Computed tomography lymphangiography via intrametatarsal pad injection is feasible in cats with chylothorax. Am. J. Vet. Res. 2022;1:1-7.
Lafond E, Weirich WE, Salisbury SK. Omentalization of the thorax for treatment of idiopathic chylothorax with constrictive pleuritis in a cat. J. Am. Anim. Hosp. Assoc. 2002;38(1):74-78.
Dickerson VM, Grimes JA, Secrest SA, et al. Abdominal lymphatic drainage after thoracic duct ligation and cisterna chyli ablation in clinically normal cats. Am. J. Vet. Res. 2019;80(9):885-890.
Radlinsky M. Thoracoscopy in the cat: an up-and-coming diagnostic and therapeutic procedure. J. Feline Med. Surg. 2014;16(1):27-33.
Clendaniel DC, Weisse C, Culp WT, et al. Salvage cisterna chyli and thoracic duct glue embolization in 2 dogs with recurrent idiopathic chylothorax. J. Vet. Intern. Med. 2014;28(2):672-677.
Bellini C, Cabano R, de Angelis LC, et al. Octreotide for congenital and acquired chylothorax in newborns: a systematic review. J. Paediatr. Child Health. 2018;54(8):840-847.
Hardie RJ, Hayashi K, DaCosta Gomez T, et al. The use of the somastostating analogue (octreotide) for the treatment of idiopathic chylothorax in dogs and cats. In; Proceedings, 13th Annual ACVS Symposium, Washington DC, 2003.
Sack D, Hyndman P, Milligan M, et al. Decortication, thoracic omentalization, and pericardiectomy for treatment of severe fibrosing pleuritis in a cat. J. Am. Vet. Med. Assoc. 2022;1:1-6.
Elizabeth Rozanski
After obtaining her DVM from the University of Illinois in 1992, Dr. Rozanski pursued a rotating internship at the University of Minnesota before following a residency at the University of Pennsylvania Read more
Lungworm and heartworm are an underestimated but potentially serious threat for many cats, as this article reveals.
Diaphragmatic hernia is a common consequence of traumatic injury in cats and may be fatal if not promptly diagnosed and treated; this article reviews the pathophysiology and treatment of the condition.
Asthma is a common disease in cats, but it can mimic many other pathologies, and the diagnosis and treatment of the condition can be challenging, as this paper explains.
Lymphoma is one of the most common neoplasms of cats, and the mediastinal form can be a major differential for a cat that presents with respiratory signs, as James Elliott describes.