
Feline lungworm and heartworm
Lungworm and heartworm are an underestimated but potentially serious threat for many cats, as this article reveals.
Issue number 32.2 Other Scientific
Published 16/11/2022
Also available in Français , Deutsch , Italiano and Español
Lymphoma is one of the most common neoplasms of cats, and the mediastinal form can be a major differential for a cat that presents with respiratory signs, as James Elliott describes.

Lymphoma is one of the most common feline neoplasms, and should be high on the differential diagnosis list for a cat with almost any mass.
Mediastinal lymphoma can involve the thymus and regional lymph nodes, and most affected cats will present with signs of thoracic disease, including a degree of dyspnea.
Initial management revolves around stabilization and emergency management of the patient, followed by diagnostic tests and appropriate chemotherapy.
Medical treatment options for mediastinal lymphoma are typically highly effective, and clinical signs will usually resolve very rapidly, with a survival prognosis beyond one year with suitable chemotherapy.
Lymphoma (historically often termed lymphosarcoma; LSA) represents a heterogeneous group of neoplasms that originate from lymphocytes. The neoplasms usually arise in lymphoid tissues such as lymph nodes, bone marrow and spleen, but they may develop in almost any tissue in the body due to the widespread distribution and migratory nature of lymphocytes. Lymphoma is one of the most common neoplasms seen in the cat and should be high on the differential diagnosis list for a cat with almost any mass.
Over time, a significant change in the epidemiology and clinical characteristics of lymphoma in cats has coincided with the integration of feline leukemia virus (FeLV) testing and elimination programs of the late 1970s and 1980s, and this was further modified by the appearance of FeLV vaccines in the late 1980s. The decline in FeLV-associated lymphoma mirrors the reduced incidence of FeLV infection. Interestingly, despite this, the overall prevalence of feline lymphoma is upwards; this seems to be mainly due to an increased frequency of the gastrointestinal form of lymphoma, as well as lymphoma in other anatomic sites 1.
The true incidence of feline lymphoma is unknown. There is no typical signalment for cats with lymphoma because it varies widely based on anatomic site and FeLV status. Siamese cats have been suggested to be at increased risk of lymphoma, and may even develop distinctive subtypes of the disease with a unique biologic behavior 2.
FeLV was historically the major cause of feline lymphoma, and most cases were associated with active infection. This often occurred in young cats, with a median age of around 3 years. In addition, there were certain anatomic subtypes heavily associated with FeLV infection, including the mediastinal form. However, given the dearth of FeLV these days, there has been a big shift in lymphoma cases, and this disease now affects significantly older cats, with a predominance in certain anatomic sites, such as gastrointestinal lymphoma.
FeLV is directly involved in lymphomagenesis, as it inserts into the cat’s genome, resulting in cell proliferation and altered gene expression 1. Feline immunodeficiency virus (FIV) infection can increase the risk of lymphoma in cats, although here evidence suggests an indirect role, secondary to the immunosuppressive effects of the virus. FIV associated lymphoma is more likely to be of B-cell type, as opposed to the T-cell predominance associated with FeLV 3.
A predisposition of the oriental cat breeds to develop lymphoma suggests a potential heritable genetic predisposition 2.
There is some data to suggest an increased risk of lymphoma in cats exposed to environmental tobacco smoke (ETS) 4.
As well as the increased risk of lymphoma in cats with the immunosuppressive FIV infection, there is also evidence that pet cats receiving cyclosporine following renal transplantation have an increased risk of cancer, including lymphoma 5.
There is a suggested link between intestinal lymphoma and inflammatory bowel disease, and a potential association between Helicobacter infection and gastric mucosa-associated lymphoid tissue (MALT) lymphoma in cats, which is a recognized syndrome in humans. One study in cats found statistically significant increases in the prevalence of mucosa-invading bacteria and intravascular bacteria in large cell lymphoma biopsy samples 6. There is a suggestion that chronic inflammation from injection sites may increase the risk of developing subcutaneous lymphoma in cats 7.
James Elliott
The mediastinal form can involve the thymus and regional (mediastinal, tracheobronchial and sternal) lymph nodes. Most cats present with signs of thoracic disease, due either to the space-occupying effect of the tumor, or secondary to pleural effusion, which is very common. The clinical signs associated with mediastinal lymphoma include dyspnea (80%), tachypnea, and a non-compressible cranial thorax with dull heart and lung sounds. Horner’s syndrome and cranial vena cava (caval) syndrome may be seen, with associated swelling of the head and neck due to compression of vessels draining the head. However, in the author’s experience caval syndrome is very uncommon in cats with mediastinal lymphoma, and much more common in canine mediastinal lymphoma/thymoma. Hypercalcemia occurs frequently with mediastinal lymphoma in dogs, but is actually very rare in cats.
Most patients present with some degree of dyspnea, and initial management revolves around stabilization and emergency management until they are comfortable enough to undergo diagnostics. This can involve oxygen supplementation with minimal handling to reduce stress, and sedation or analgesia (e.g., butorphanol) if indicated. There should be rapid assessment to verify if pleural effusion is present (ultrasonography, radiography); if there is a large volume of fluid this must be drained quickly, as it contributes significantly to the dyspnea.
The disease is confined to the mediastinum in most cases, although there can certainly be involvement of other regional nodal groups or distant sites. The author has commonly seen involvement of prescapular or even mandibular lymph nodes, particularly later in the disease course, often at the time of relapse. The author has also seen a few cases that initially present with a large mass that has appeared suddenly in the prescapular region. This has ultimately been demonstrated by computed tomography (CT) to be contiguous with a large mediastinal mass, as opposed to actually being the prescapular lymph node.
The majority of cats with mediastinal lymphoma in older reports were young (median age, 2-4 years), FeLV positive, and had a T-cell immunophenotype tumor. However, as expected with the decline of FeLV, the typical phenotype has altered. In a recent UK study of 55 cats with mediastinal lymphoma, the majority (>90%) were antigenically FeLV/FIV negative, young (median age, 3 years), male (3.2:1 male-to-female ratio), and nearly one-third were of the Siamese breed 8. Immunophenotype was not reported, probably as it is performed less in cats. This is likely because most studies suggest that, unlike in dogs, immunophenotype appears to have less prognostic significance in cats.
A form of mediastinal lymphoma also occurs primarily in young, FeLV-negative Siamese cats that appears to be less biologically aggressive and more responsive to chemotherapy than FeLV-associated forms.
Thoracic radiographs may identify an obvious mediastinal mass (Figure 1), although sometimes the presence of significant pleural effusion can make it difficult or impossible to visualize prior to drainage (Figure 2) and repeat radiographs or ultrasound may be necessary (Figure 3). CT may be helpful, as a mass can be seen irrespective of the presence of effusion; however, this imaging modality generally does not contribute to a definitive diagnosis, because there are several differentials for a cat with a mediastinal mass.

Figure 1. A lateral thoracic radiograph of a cat; note the ovoid soft tissue mass overlying sternebrae 2-4, cranial to the heart. This was cytologically confirmed to be lymphoma.
© James Elliott

Figure 2. A lateral thoracic radiograph of a cat showing a moderate volume of pleural effusion. Note the scalloped lung edges due to pleural fluid and the lack of detail in the cranial mediastinum, as well as the loss of the cardiac outline. Post-drainage, a cranial mediastinal mass was visible. In this case, the mass did not require sampling, as cytology of the pleural fluid was consistent with large cell lymphoma.
© James Elliott

Figure 3. A thoracic ultrasound scan from the cat in Figure 2. After drainage, breathing was significantly improved, and a hypoechoic mass could be visualized.
© James Elliott
Fine-needle aspirate (FNA) cytology of the mass or cytologic evaluation of pleural fluid may be sufficient to establish a diagnosis. In most cats, lymphoma exfoliates well with a fine-needle aspiration, and the finding of a monomorphic population of intermediate or large lymphoid cells will confirm the diagnosis (Figure 4). On occasion, a definitive diagnosis of lymphoma in cats with a mediastinal mass can be more challenging.
A major differential for mediastinal lymphoma is thymoma. The cytologic features of thymoma can be distinct from lymphoma in many cases, but the diagnosis can be challenging because of a preponderance of small lymphocytes in thymoma. Mast cells can also be seen in up to 50% of aspirates from thymomas (Figure 5). The addition of immunophenotypic and clonality assessment may be helpful in equivocal cases.

Figure 4. Cytology from a cytospin preparation of pleural fluid from the cat in Figures 2 and 3. Note the monomorphic population of very large, round cells with features of immature lymphoblasts, and the intense blue cytoplasm, coarse open chromatin with multiple nucleoli and perinuclear clear zone. Also note the solitary eosinophil (yellow arrow), mitotic figures (green arrow) and lymphoglandular bodies (red arrows).
© James Elliott

Figure 5. Cytology from a fine-needle aspirate of a mediastinal mass in a cat which was ultimately surgically removed and shown to be a thymoma. The predominant cell population is small, mature lymphocytes with a thin rim of cytoplasm and dark, condensed purple nuclei. In addition, there are scattered epithelial cells (long black arrow) and two mast cells (short black arrows). This is a classic cytology for thymoma, with a predominance of small mature lymphocytes admixed with epithelial cells and mast cells. This is in contrast to lymphoma, where a monomorphic population of large, immature lymphocytes are seen, as in Figure 4.
© James Elliott
Where the diagnosis is equivocal, potential additional diagnostics could include:
Finally, Tru-Cut biopsy can be useful for large masses which communicate with the chest wall (to ensure there is a low risk of causing iatrogenic pneumothorax), but in the author’s practice this option is rarely required nowadays.
Chemotherapy is by far the most utilized treatment option for cats with mediastinal lymphoma. Generally, lymphoma is considered a systemic disease, even if it appears to be localized at diagnosis. This means that although a cat with localized lymphoma (e.g., mediastinal lymphoma) might appear disease-free in other anatomic sites based on imaging (or even cytology, e.g., of the liver or spleen), it is considered likely that they will have cancer cells in these locations at a microscopic level. Therefore, the goal of cytotoxic chemotherapy is to treat both the known macroscopic disease, but also any occult, microscopic disease.
Surgery is not indicated in cats with mediastinal lymphoma, for the reasons outlined above and the morbidity and risk associated with thoracic surgery. Wound healing would also delay the instigation of chemotherapy. In addition, medical treatment options are typically (at least initially) highly effective, and lymphoma responds very rapidly. Therefore, whilst pets with some tumor types will rapidly improve clinically with surgical removal, this is not the case in mediastinal lymphoma.
Most cats with lymphoma at any site, including mediastinal, will be offered either a COP (cyclophosphamide, vincristine (oncovin) and prednisolone/prednisone) or CHOP (COP plus doxorubicin (hydroxydaunorubicin)) protocol, as shown in Tables 1 and 2. CHOP-type protocols are the standard of care in humans with the most common types of lymphoma. Similarly, canine lymphoma (particularly of the B-cell type) is typically treated first-line with a CHOP (i.e., doxorubicin-inclusive) protocol by most oncologists. The best option for feline lymphoma at any site is less clear-cut, and both COP and CHOP protocols are widely utilized, with most studies failing to demonstrate that CHOP is significantly superior to COP. In addition, doxorubicin appears to be less effective as a single agent in cats compared to dogs, and nephrotoxicity is a possible adverse effect in cats. Given the propensity for chronic kidney disease in ageing cats, this must be considered when making a therapeutic plan. Doxorubicin is also an extreme vesicant, causing potentially extensive tissue sloughing in the event of extravasation, so feline patients may require sedation for safe administration, depending on temperament. Doxorubicin is, however, very unlikely to cause cardiotoxicity in cats at standard doses and schedules.
Table 1. A standard COP (cyclophosphamide, vincristine (oncovin) and prednisolone/prednisone) protocol for cats.
| Drug | Week 1 | Week 2 | Week 3 | Week 4 | Weeks 7,10,13,16,19,22,25 |
|---|---|---|---|---|---|
| Vincristine | x | x | x | x | x |
| Cyclophosphamide | x | x | x | ||
| Prednisolone | x | x | x | x | x |
| Providing the patient is in remission at week 25, chemotherapy (including prednisolone) is ceased. If complete remission has not been achieved by week 7 (i.e., after the more intense induction period of weeks 1-4), additional or alternative therapies should be considered. Historically, continuous COP-based chemotherapy schedules have been recommended. In the author’s experience, cats in remission after 6 months of therapy can be treated with discontinuous schedules as above. | |||||
| Vincristine: 0.7 mg/m2 IV; Cyclophosphamide: 250 mg/m2 IV/PO; Prednisolone: 2 mg/kg PO q24h for 14 days then 1 mg/kg q48h | |||||
Table 2. A standard CHOP (COP plus doxorubicin (hydroxydaunorubicin)) protocol for cats.
| Week | 1 | 2 | 3 | 4 | 6 | 7 | 8 | 9 |
| Vincristine | x | x | x | x | ||||
| Cyclophosphamide | x | x | ||||||
| Doxorubicin (or epirubicin) | x | x | ||||||
| Prednisolone | x | x | x | x | x | x | x | x |
| Week | 11 | 13 | 15 | 17 | 19 | 21 | 23 | 25 |
| Vincristine | x | x | x | x | ||||
| Cyclophosphamide | x | x | ||||||
| Doxorubicin (or epirubicin) | x | x | ||||||
| Prednisolone | x | x | x | x | x | x | x | x |
| Vincristine: 0.7 mg/m2 IV; Cyclophosphamide: 250 mg/m2 IV/PO; Doxorubicin or epirubicin: 1 mg/kg or 25 mg/m2 IV; Prednisolone: 2 mg/kg/day, week 1; 1.5 mg/kg/day week 2; 1.0 mg/kg/day week 3; thereafter 0.5 mg/kg/day PO | ||||||||
A retrospective study of cats with mediastinal lymphoma treated with either COP or CHOP protocols demonstrated an overall response rate of 95%, with an overall median survival time (MST) of just over a year (and 980 days if complete response is achieved) 8. Complete response (CR) and partial response (PR) rates did not differ significantly between COP and CHOP protocols, with overall median survival reported as 373 days (range 20-2015 days). Cats achieving CR survived longer (median 980 days vs. 42 days for PR). Age, breed, sex, location (mediastinal vs. mediastinal plus other sites), viral status and steroid pre-treatment did not affect response or survival. The prevalence of FeLV positive cats in this study was low (9%), with males and young Siamese cats appearing to be over-represented.
In contrast, mediastinal lymphoma in young FeLV-positive cats is generally associated with a poor prognosis, and MSTs of approximately 2 to 3 months can be expected after treatment with either CHOP or COP protocols. Slightly more promising results were obtained in a recent, small retrospective Brazilian study, where cats with mediastinal lymphoma (from a 90% FeLV positive population) had a MST of approximately 7 months using a novel protocol consisting of vincristine, prednisolone, doxorubicin and lomustine 9.
Chemotherapy should not be thought of as a “formula”, and whilst protocols are useful as a starting point, they should be modified for the individual. Adverse effects can include gastrointestinal upset, myelosuppression (principally neutropenia) and – rarely – drug-specific toxicity such as doxorubicin-induced renal injury. An awareness of the patient’s history, previous response to chemotherapy and any adverse effects, and appropriate blood tests are required in an effort to maintain the optimum dose intensity – i.e., in deciding whether the chemotherapy dose should be increased, reduced or maintained. Most clinicians will proceed with chemotherapy providing the absolute neutrophil count (not the total white cell count!) is greater than 2.5 x 109/L, but it may be safe to proceed if the count is lower than this, depending on various factors. There is really no definitive point at which the neutrophil count suggests that it is safe to continue with a given protocol, and different clinicians will have different experiences, and some clinicians may have different cut-offs for different drugs. For example, doxorubicin is a particularly myelosuppressive drug which can cause severe neutropenia, so if used some oncologists will have a higher “threshold” for the neutrophil count before happily proceeding with the next dose. Equally, some clinicians may be more cautious if they are treating a frail patient, if they have experienced severe neutropenia previously, or if the pet owner has major concerns regarding possible adverse effects. Conversely, if there is no neutropenia/myelosuppression at all and no clinical adverse effects, some clinicians may consider a dose increase for subsequent treatments of the chosen drug. A recent study showed that in dogs receiving a 19-week CHOP protocol for lymphoma, treatment proceeded as long as the neutrophil count was >1.5 x 109/L; this reduced the number of dose delays and did not result in a significant increase in adverse effects. Whilst such data is not currently published for cats, it is likely that a “safe” threshold for chemotherapy may be less than 2.5 x 109/L, but a significant neutropenia may require drug dose reduction or increased dosing interval. So if a cat’s neutrophil count is below the chosen cut-off when a dose is due, a 2-7 day delay (depending on the magnitude of the neutropenia) should be instituted. If this continues for future doses or the neutropenia is severe, then a dose reduction may be warranted for future doses.
This exemplifies the “art” of chemotherapy, which comes partly with experience but also over time treating the individual patient, and indeed most cats tolerate chemotherapy well. So with appropriate experience and skill, drug or dose modifications, dose reductions or holidays, drug frequency alterations and anti-emetic prophylaxis, cats can enjoy an excellent quality of life whilst receiving chemotherapy. Of note, cats appear resistant to cyclophosphamide-induced cystitis and doxorubicin-induced cardiotoxicity, and they rarely become septic even with severe drug-induced neutropenia. Multiple studies report that the majority of owners are happy with their pet’s quality of life whilst receiving chemotherapy for lymphoma 10 (Figure 6).
Figure 6. Cats can enjoy an excellent quality of life whilst receiving chemotherapy.
© Riccardo Finotello, University of Liverpool
Where clinical signs reappear, various rescue chemotherapy protocols are available, utilizing different drugs to which the tumor cells have not yet been exposed (Table 3). Unfortunately, there is often intrinsic chemoresistance or acquired cross-resistance to many of these drugs. Many cats are very symptomatic when they relapse, which may allow less time to try various rescue protocols in order to determine the most effective regime. Response rates are usually modest and typically not durable, although in pets that do develop a strong partial or complete response, outcome is significantly improved.
Table 3. Common “rescue” chemotherapy protocols for recurrence of feline lymphoma.
| Drug(s) | Typical response rate | Median remission time |
|---|---|---|
| Lomustine, methotrexate and cytarabine | 46% | 61 days |
| MOPP (mechlorethamine, vincristine, procarbazine, prednisolone) | 70% | 166 days |
| MOMP (mechlorethamine, vincristine, melphalan, prednisolone) | 58% | 39 days |
| DMAC (dexamethasone, melphalan, actinomycin D, cytarabine) | 26% | 14 days |
| Lomustine (CCNU) | 54% | 39 days |
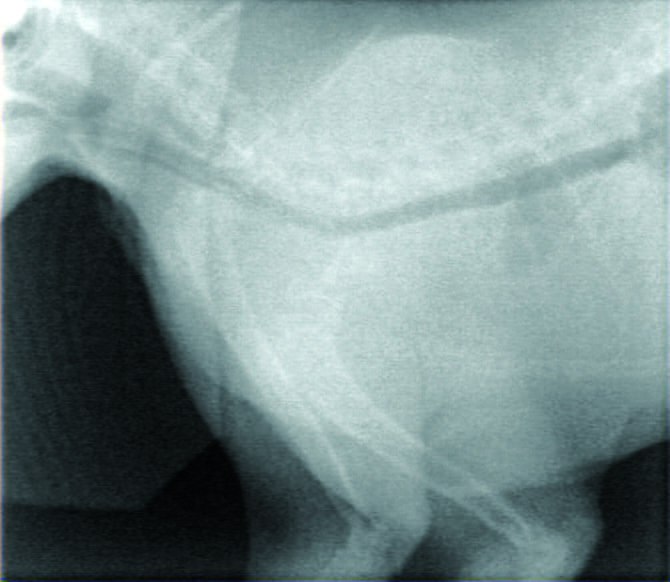
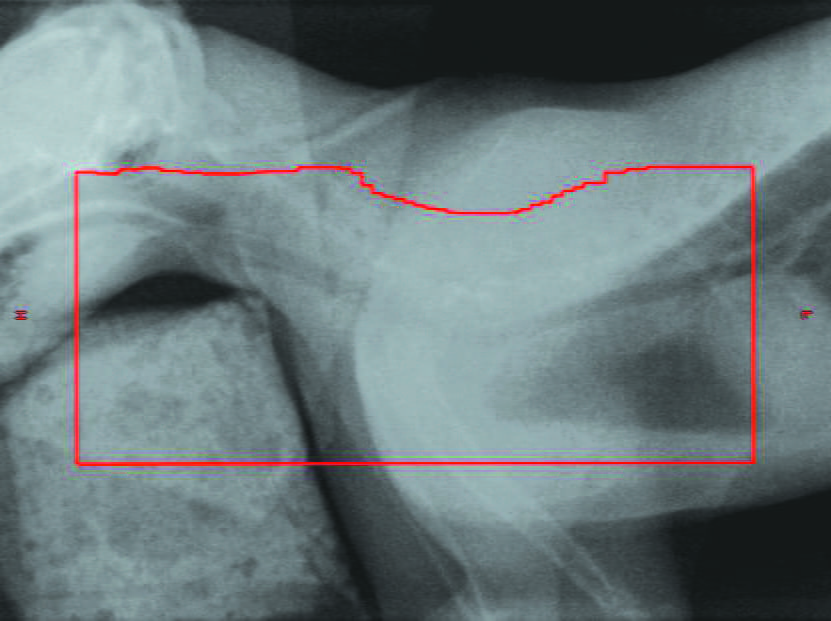
Radiotherapy has been commonly used very successfully for certain types of solitary feline lymphoma, particularly nasal lymphoma, yet interestingly it has seldom been used for mediastinal lymphoma. The reasons for this are probably multifactorial, including the previous association with FeLV and a poor prognosis, the scarcity of available treatment centers, potentially poor (repeated) anesthetic candidacy, difficulty in tumor targeting due to respiratory motion, large volumes of pleural effusion, large tumors and the perceived radiation sensitivity of normal intrathoracic tissues near the tumor (particularly the pericardium, heart and lungs). Lymphocytes are exquisitely sensitive to radiation and die very quickly, and lower doses are often required to effectively treat lymphoma than most other tumor types. Therefore, with the advent of more sophisticated radiation facilities, this therapy may become a potential treatment resource. For example, patients with mediastinal lymphoma often relapse in the mediastinum, so radiotherapy alone, or in combination with chemotherapy, may more effectively eradicate neoplastic lymphocytes than chemotherapy alone, and could become part of definitive-intent, first-line treatment. To date, the author has mainly used radiotherapy as a palliative-intent treatment for relapsed cases following initial treatment with systemic chemotherapy, with good (albeit temporary) results (Figure 7).
 |
| a |
 |
| b |
Figure 7. “Port film” radiographs taken of a cat with mediastinal lymphoma being treated with palliative-intent radiotherapy, which had previously responded to CHOP chemotherapy, but had relapsed in the mediastinum and mandibular/prescapular nodes a few months later. There was no response to re-introduction of chemotherapy. The pre-treatment radiograph (a) shows the absence of cardiac silhouette and pleural effusion. By the final treatment, only 4 days later (b), there was a complete radiographic response to treatment. The red line denotes the area that was treated with radiotherapy.
© James Elliott
Cats with mediastinal lymphoma mostly present with relatively acute-onset respiratory signs and often require emergency triage and management, although a diagnosis is relatively easily achieved. These days, cats with mediastinal lymphoma are usually FeLV negative and can have a survival prognosis of over a year with suitable chemotherapy. In cats achieving a complete remission, duration of remission can be very durable (>2.5 years). A subset of younger, male, FeLV negative oriental cats can have a particularly good prognosis, but most cats will respond favorably to chemotherapy and can have a good quality of life on treatment.
Neil JC, Onions DE. Feline leukaemia viruses: molecular biology and pathogenesis. Anticancer Res. 1985;5(1):49-63.
Gabor LJ, Malik R, Canfield PJ. Clinical and anatomical features of lymphosarcoma in 118 cats. Aust. Vet. J. 1998;76(11):725-732. DOI:10.1111/j.1751-0813.1998.tb12300.x
Kaye S, Wang W, Miller C, et al. Role of Feline Immunodeficiency Virus in lymphomagenesis – going alone or colluding? ILAR J. 2016;57(1):24-33. DOI:10.1093/ilar/ilv047
Bertone ER, Snyder LA, Moore AS. Environmental tobacco smoke and risk of malignant lymphoma in pet cats. Am. J. Epidemiol. 2002;156(3):268-273. DOI:10.1093/aje/kwf044
Wormser C, Mariano A, Holmes ES, et al. Post-transplant malignant neoplasia associated with cyclosporine-based immunotherapy: prevalence, risk factors and survival in feline renal transplant recipients. Vet. Comp. Oncol. 2016;14(4):e126-e134. DOI:10.1111/vco.12120
Hoehne SN, McDonough SP, Rishniw M, et al. Identification of mucosa-invading and intravascular bacteria in feline small intestinal lymphoma. Vet. Pathol. 2017;54(2):234-241. DOI:10.1177/0300985816664792
Roccabianca P, Avallone G, Rodriguez A, et al. Cutaneous lymphoma at injection sites: pathological, immunophenotypical, and molecular characterization in 17 cats. Vet. Pathol. 2016;53(4):823-832. DOI:10.1177/0300985815623620
Fabrizio F, Calam AE, Dobson JM, et al. Feline mediastinal lymphoma: a retrospective study of signalment, retroviral status, response to chemotherapy and prognostic indicators. J. Feline Med. Surg. 2014;16(8):637-644. DOI:10.1177/1098612X13516621
Horta RS, Souza LM, Sena BV, et al. LOPH: a novel chemotherapeutic protocol for feline high-grade multicentric or mediastinal lymphoma, developed in an area endemic for feline leukemia virus. J. Feline Med. Surg. 2021;23(2):86-97. DOI:10.1177/1098612X20926893
Thornton LA, Cave N, Bridges JP, et al. Owner perceptions of their cats quality of life when treated with a modified University of Wisconsin-Madison protocol for lymphoma. J. Feline Med. Surg. 2018;20(4):356-361. DOI:10.1177/1098612X17710844
James Elliott
Dr. Elliott graduated from the University of Edinburgh and worked in general practice before completing an internship and residency in small animal oncology at the University of Liverpool Read more
Lungworm and heartworm are an underestimated but potentially serious threat for many cats, as this article reveals.
Diaphragmatic hernia is a common consequence of traumatic injury in cats and may be fatal if not promptly diagnosed and treated; this article reviews the pathophysiology and treatment of the condition.
Chylothorax is a differential for any cat with pleural effusion; here Elizabeth Rozanski describes her preferred approach to such cases.
Asthma is a common disease in cats, but it can mimic many other pathologies, and the diagnosis and treatment of the condition can be challenging, as this paper explains.