
Feline lungworm and heartworm
Lungworm and heartworm are an underestimated but potentially serious threat for many cats, as this article reveals.
Issue number 32.2 Other Scientific
Published 23/11/2022
Also available in Français , Deutsch , Italiano and Español
Asthma is a common disease in cats, but it can mimic many other pathologies, and the diagnosis and treatment of the condition can be challenging, as this paper explains.

Feline allergic asthma is common, but the clinical signs and radiographic features mimic other respiratory disorders.
Comprehensive evaluation – to rule out other diseases – and ultimately obtaining an airway lavage will help to increase confidence in diagnosis.
Treatment focuses on environmental modification, weight management, glucocorticoids and – if bronchospasm is present – bronchodilators.
The prognosis ranges from guarded to good, depending on if a cat presents primarily with a cough or life-threatening asthma attacks, and is linked to response to therapy.
Feline allergic asthma is a common reason for cats to present for veterinary care, and manifests as a cough, wheeze and episodic respiratory distress, the latter associated with increased expiratory effort (“abdominal push”). An asthma “syndrome” has been recognized in cats for over 100 years, and is reported worldwide, with an estimated 1-5% of the pet cat population affected 1. The onset of asthma is typically early in life, although cats with milder clinical signs may not obtain veterinary care until they are middle-aged, as the condition tends to be progressive, especially without medical care. All breeds of cats are potentially susceptible, although there is a possible predisposition in the Siamese breed.
Allergic asthma occurs in genetically predisposed cats with certain environmental exposures 2. Specifically, allergic asthma is an example of a type I hypersensitivity reaction to inhaled aeroallergens, in which T helper 2 lymphocytes orchestrate an immune response that damages the airways. Collectively, the immune response promotes airway eosinophilia, mucus hypersecretion, airway hyperresponsiveness (the tendency of the airways to constrict more robustly in response to non-specific triggers compared with a healthy cat), bronchospasm (which is at least partially reversible with time or treatment), and airway remodeling.
Disease mimics can present with clinical signs of cough, wheeze and expiratory respiratory distress (especially with increased expiratory effort), and have survey thoracic radiography with a bronchial or bronchointerstitial pattern, include heartworm-associated respiratory disease (HARD) caused by immature L5 larvae of Dirofilaria immitis and the host immune response, Aelurostrongylus abstrusus (a metastrongyloid nematode) and Toxocara cati (specifically from pulmonary migration of this common nematode). Additionally, for coughing cats, especially if they are older at first onset of clinical signs, and have a bronchocentric radiographic pattern, chronic bronchitis is a top consideration. This is an inflammatory disease caused by varying insults that damage airways and impair mucociliary function, and is characterized by airway neutrophilia 3. Cats presenting in respiratory distress (but not predominantly with increased expiratory effort) or open-mouth breathing, especially if a heart murmur is heard on auscultation, may have congestive heart failure. Finally, an important but uncommonly recognized group of disorders, known as bronchiolar disorders (or small airway diseases), can mimic asthma 4. Bronchiolar diseases have no pathognomonic clinical signs and cannot be visualized on radiography; computed tomography (CT) of the thorax and ultimately lung biopsy are required to identify and characterize the specific type of disorder. One subtype, constrictive bronchiolitis obliterans, closely resembles features seen in cats presenting in status asthmaticus (life-threatening asthma attack).
While not strictly “diagnostic tests”, consideration of the signalment, owner-reported clinical signs and physical examination findings form the first essential piece of reaching a diagnosis of feline allergic asthma. There is no single test to make a definitive diagnosis, but supporting data will help rule out or make less likely other disease mimics and put asthma higher on the differential list. As mentioned above, when the first signs are noted at a young age (even if the cat only presents for veterinary treatment later in life), this is more supportive of asthma and many of the parasitic bronchial disorders. When onset occurs later in life, chronic bronchitis is more typical.
Thoracic radiography is one of the first and most common diagnostic tests performed in any cat presenting with respiratory clinical signs. It is important to note that normal thoracic radiographs have been reported in roughly a quarter of cats with lower airway disease 5. Typically, pathologic lesions are bronchocentric, including a bronchial or bronchointerstitial pattern (Figure 1). In some of the parasitic diseases, patchy interstitial patterns may be prominent, and the cranial or caudal pulmonary arteries enlarged. In cats presenting in status asthmaticus, air trapping, manifesting as lung fields with increased volume and decreased opacification, is noted (Figure 2). In these cases, the diaphragm may be flattened, with increased distance between the caudal border of the cardiac silhouette and the diaphragm on the lateral projection. Any respiratory disorder leading to mucus hypersecretion can lead to plugging of lobar bronchi (most commonly in the right middle lung lobe or the caudal portion of the left cranial lung lobe) and resultant atelectasis of the affected lobe. Radiography may also be used to rule out a wide variety of other cardiopulmonary disorders (e.g., metastatic neoplasia, pleural effusion).

Figure 1a. A lateral thoracic radiograph from a 6-year-old male neutered Domestic Shorthair cat with asthma. A diffuse bronchial pattern is visible within the lung field.
© Dr. Carol Reinero.

Figure 1b. A lateral thoracic radiograph from a 6-year-old male neutered Domestic Shorthair cat with asthma. The magnified view displaying a thickened airway wall (“donut”) in cross-section (arrowed).
© Dr. Carol Reinero.
 |
| a |
 |
| b |
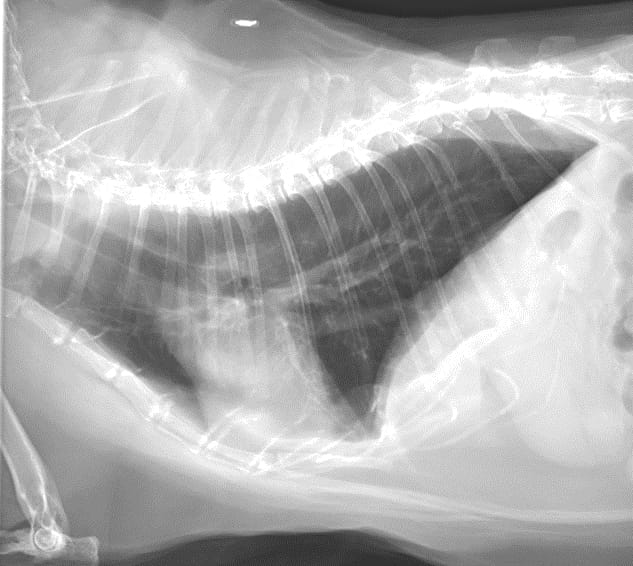
Figure 2. Lateral (a) and dorsoventral (b) radiographs from a 2-year-old female spayed Siamese cat with asthma. In both projections there is a moderate diffuse bronchial pattern with hyperinflated lungs. Note the tenting of the diaphragm on the dorsoventral projection.
© Dr. Carol Reinero.
Use of point-of-care lung ultrasound in cats with labored respiration is becoming more commonplace in both general and specialty practice 6. Ultrasonography can detect pleural cavity disorders including pneumothorax (indicated by a lack of a glide or slide sign) and pleural effusion (hypoechoic fluid). Signs of cardiac disease, which is beyond the spectrum of this paper, may be evident. Additional lung abnormalities include B lines, nodule sign, tissue sign, shred sign, and wedge sign. Cats with asthma as a cause of their respiratory signs should have an absence of all the aforementioned abnormalities (typically termed “dry lung”; (Figure 3)) with the possible exception of a tissue sign in the region of a lobe that has undergone atelectasis from mucus plugging.

Figure 3. A lung ultrasound performed in a 4-year-old male neutered Domestic Shorthair cat with suspected asthma. This image represents a picture of “dry” lung, whereby no pathology is seen coming off the lung line (white arrowheads). The rib heads and their shadows to the far field are denoted by the white arrows.
© Dr. Carol Reinero.
A complete blood count may show eosinophilia, which is compatible with either asthma or parasitic disease, but the absence of peripheral eosinophilia does not rule out airway eosinophilia. There are no findings on serum biochemical profile or urinalysis that help in the diagnosis of asthma; however, if a cat is to undergo general anesthesia for advanced imaging and/or airway lavage, knowledge of overall health status and organ function is important.
Ancillary testing for parasitic diseases should include fecal flotation, fecal Baermann, and, in endemic regions, heartworm antibody and antigen tests 7. Toxocara cati may be missed by fecal flotation if lung migration is occurring in the prepatent period. It is generally recommended that fecal Baermann testing for Aelurostrongylus abstrusus is repeated up to three times, as the larvae may be intermittently coughed up and swallowed to subsequently appear in the feces. It may be less expensive to try a course of an appropriate anthelmintic in lieu of specific parasitic testing.
While not commonly performed in patients suspected of having feline asthma, thoracic CT can be extremely useful, and is the best imaging modality to identify bronchiolar disorders that may mimic asthma 4. CT may be used in cases where initial investigations are not adequate to provide a diagnosis, as it has a high sensitivity for identifying a wide variety of pulmonary, vascular, pleural cavity and cardiac disorders 8.
Bronchoscopy, a modality that allows visual inspection of the lumen of the tracheobronchial tree, rarely adds important diagnostic information in asthmatic cats. Most changes are non-specific and diffuse in affected individuals. Additionally, while bronchoalveolar lavage (BAL) can be performed using a bronchoscope, the blind technique is preferred as it can be done quickly in general practice with minimal equipment. BAL is strongly recommended as a diagnostic to help confirm asthma, with the typical gross appearance on sampling being slightly opaque fluid with a foamy white layer of surfactant on top (Figure 4). An advised technique is shown in Box 1. The BAL sample should be submitted for cytologic examination and culture; in cases where Mycoplasma spp. cannot be cultured, a PCR can be performed instead. The presence of increased eosinophils in BAL supports either parasitic diseases or allergic asthma, and underscores the importance of trying to rule out a parasitic etiology with testing or anthelmintic trials prior to airway lavage. Cytology examination that suggests non-septic suppurative inflammation supports a diagnosis of chronic bronchitis. Septic, suppurative inflammation, especially where there is a positive culture of a clinically relevant bacterial species, can reflect secondary bacterial infection to any primary lower airway disease. While secondary bacterial infections are not common, they do have specific targeted therapy and are therefore important to recognize.

Figure 4. Bronchoalveolar lavage fluid immediately post-collection. The retrieved fluid is slightly opaque, with the top layer showing foamy surfactant, the latter indicative of a deep wash.
© Dr. Aida Vientos-Plotts.
Box 1. Bronchoalveolar lavage (BAL) technique.
|
Less commonly performed diagnostics include pulmonary function testing and allergy testing (either serum allergen-specific IgE testing 9 or intradermal testing). In humans with allergic asthma, pulmonary function testing (spirometry) is a primary means of diagnosis and therapeutic monitoring, but since this requires patient compliance to forcibly exhale through a mouthpiece, the test is not practical for cats. There are alternative means to investigate pulmonary mechanics, but they require specialized equipment and expertise and thus are mostly used in research settings. In contrast, allergy testing (specifically the serum test) is widely available and may help guide allergen-avoidance strategies.
The treatment of feline asthma should be tailored to the clinical presentation, so will differ between unstable cats presenting with status asthmaticus or overt respiratory distress and cats that are stable and have less severe clinical signs (generally cough, but also wheeze or mild to moderate exercise intolerance). The general strategies for cats presenting in status asthmaticus are oxygen supplementation, minimal handling/restraint, sedatives (to facilitate an improved breathing strategy) and administration of a bronchodilator (with or without a glucocorticoid) while letting the cat calm down in a cage with privacy. The general approach to clinically stable cats with mild to moderate signs include glucocorticoids and, in some cases, bronchodilators. For all asthmatic cats, strategies to modulate the environment and to promote weight loss (if over-conditioned) are generally applicable.
Cats presenting with a life-threatening asthma attack (status asthmaticus) must be treated with a bronchodilator. The preferred route for these critical cases is by injection (e.g., terbutaline at 0.01 mg/kg SC or IM), as severe bronchospasm limits delivery of inhaled bronchodilators to the lower airways. If this is not possible, an inhaled bronchodilator (e.g., albuterol) can be given via metered-dose inhalant with a spacer (90 mcg/puff, two puffs) and repeated in 15-20 minutes, on the assumption that the first dose allows some bronchodilation which then permits the second dose to better reach its target site of action. Other important strategies for cats in this category include minimal handling, oxygen supplementation (including a place to hide and calm down), and in some cases, a sedative. Glucocorticoids should also be given, but generally take longer to work, underscoring the importance of a rapidly acting bronchodilator to reverse airflow limitation.
Once cats are no longer in crisis and their clinical signs are stable, they should be treated as outlined below (“Treatment of stable cats”). One notable difference is that cats with episodes of status asthmaticus are prone to repeated asthma attacks, and bronchodilator therapy should be considered as an important part of their long-term medical management. Bronchodilators are typically from two major classes of drugs, methylxanthines and beta-2 agonists (the latter being available as either short- or long-acting). Methylxanthines are typically administered orally, and theophylline as a 100 mg extended-release tablet or capsule is a popular choice due to its every day or every other day administration. Short-acting beta-2 agonists are potent and work rapidly, and are available as oral medications or by inhalation (metered dose inhalant to be used with a spacer or nebulization). Inhalant long-acting beta-2 agonists are used commonly in people with asthma in combination with an inhaled glucocorticoid, but there is minimal data showing their efficacy in feline asthmatics. As they are less potent, they are not recommended for a cat having an asthma attack. Overall, oral bronchodilators are preferred for regular, everyday use, whereas inhaled or injectable bronchodilators can be used as “rescue” medications in emergency situations. Regular, repeated use of racemic mixtures of short-acting beta-2 agonists (e.g., R, S albuterol, known as salbutamol in some countries) have been associated with paradoxical exacerbation of airway inflammation in cats due to negative effects of the S-enantiomer 10. If regular use of a metered dose inhalant short-acting beta-2 agonist is desired, levalbuterol (i.e., R-enantiomer) is commercially available and is devoid of the S-enantiomer. Depending on national recommendations, owners can also be taught to administer injectable terbutaline in emergency situations if the cat does not tolerate inhaled bronchodilators.
As mentioned above, non-specific strategies to modulate the environment and address obesity are broadly applicable to all asthmatic cats as part of long-term management. Inhalation of allergens (both indoor and outdoor allergens) and irritants from the environment can trigger clinical signs in susceptible cats. Allergens can directly cause clinical signs via type I hypersensitivity reactions (as discussed above), and irritants can non-specifically trigger airway hyper-reactivity. If allergens can be identified using specific IgE testing, avoidance (when possible) or decreasing exposure is prudent. For example, during seasons with high outdoor allergen exposure, a cat sensitive to Bermuda grass could be kept indoors with the windows closed in an attempt to avoid or at least reduce the allergenic load. If the cat is allergic to an indoor allergen such as house dust mite, using high efficiency particulate air (HEPA) filters (both as standalone units and also in vacuum cleaners), encasing pillows and bedding with mite-proof covers, and washing such items regularly in hot water can be helpful. For non-allergenic irritants, owners should be made aware they must minimize the cat’s exposure to smoke, aerosols, powders, and dusts. One common source of the latter is from cat litter, and switching to a different type of substrate can be beneficial. Careful questioning of owners can help identify what substances may be problematic to better educate them on how to modulate the environment.
Obesity negatively impacts the immune system and puts additional stress on the respiratory system, so asthmatic cats should be kept at an ideal or lean body weight. Obesity also impacts the dose of medications, and it is important to dose glucocorticoids and bronchodilators on estimated lean body weight.
Glucocorticoids are a critical life-long therapy in asthmatic cats, as they diminish the over-reactive immune response to aeroallergens and decrease airway inflammation, which in turn blunts airway hyperresponsiveness and remodeling. Glucocorticoids should be tapered to the lowest effective dose that controls clinical signs and, ideally, airway inflammation. Routes of administration include injection, oral and inhaled. Long-acting repositol steroids such as injectable methylprednisolone are not recommended as they become less effective over time, necessitating higher doses or more frequent injections; additionally, they increase the risk of diabetes mellitus. However, in cats that cannot receive glucocorticoids by any other route (e.g., due to temperament), this may be the only viable treatment option. The author’s preferred initial choice is an oral glucocorticoid, generally starting with prednisolone at a dose of 1-2 mg/kg/day. This formulation is inexpensive, effective, and widely available as a tablet or liquid. As both injectable and oral glucocorticoids can negatively impact systemic endocrine and immune responses, it is attractive to consider delivering high doses of steroids locally to the site of action in the lungs. Inhaled steroids, typically fluticasone, are ideal for this purpose, especially when one considers asthma is often diagnosed in young cats and glucocorticoids need to be administered life-long. The author prefers fluticasone at a dose of 220 mcg/puff twice daily through a spacer, while overlapping with oral prednisolone for the first 1-2 weeks, as inhaled steroids do not work immediately. Oral steroids can subsequently be gradually tapered until the cat is only receiving inhaled steroids. To taper inhaled steroids, if there is resolution or static improvement in clinical signs, the next prescription of the inhaler can be 110 mcg/puff twice daily. If clinical control is still reasonable, the dose can be further decreased to 44 mcg/puff twice daily thereafter. Owners must be educated that lifelong administration of glucocorticoids is required in all asthmatic cats, even if the cat does not currently show clinical signs. This is because affected cats can have subclinical airway inflammation (i.e., no clinical signs but persistent microscopic airway eosinophilia) that can continue to damage the airways and predispose to permanent architectural changes in the lungs that may ultimately be less amenable to therapy 11.
Bronchodilators may not be necessary in stable asthmatic cats that present solely for coughing, assuming glucocorticoids are effective in controlling the cough. As bronchodilators have many adverse effects (excitation, systemic hypertension, tachycardia, etc.) and the cat may require additional medications (oral or inhaled), it is important not to automatically assume this class of drug needs to be administered to every asthmatic patient. In chronic, stable individuals, a bronchodilator trial can be administered to cats that do not fully respond to environmental modifications, weight management and glucocorticoid treatment. Regular use of bronchodilators may be critical for cases with a history of episodic respiratory distress, as discussed in the above section.
Carol R. Reinero
The focus on treating asthmatic cats is two-fold; to attenuate or eliminate clinical signs affecting their quality of life (e.g., cough, exercise intolerance, respiratory distress), and to control the hallmark pathologic features of asthma (including airway inflammation, hyperresponsiveness and remodeling). These two goals do not always occur in parallel, as there can be a dissociation between clinical signs and airway inflammation 11, making it challenging for clinicians to be confident that inflammation is controlled in asymptomatic cats on glucocorticoid therapy. Repeat airway lavages, while invasive, are the only current means to determine if there is microscopic control of inflammation in these cats. However, it is important to note that if clinical signs persist, especially if moderate to severe, the current therapeutic protocol is insufficient, and changes to achieve better asthmatic control or identify comorbidities must be made.
Asthma has variable morbidity and occasional mortality, and given that it typically first appears in young cats, the requirement for lifelong management must be emphasized, which will minimize irreversible damage to the airways. Cats primarily presenting with cough typically have good responses to medical management, but those presenting with episodes of respiratory distress are more susceptible to repeated hospitalization and, in some cases, death.
Feline allergic asthma is a common respiratory disorder that must be differentiated from other disease mimics. This can be performed by considering the signalment, owner-reported clinical signs, physical exam findings, diagnostic investigations and airway lavage. Treatment is based on presentation; cats with status asthmaticus should receive a bronchodilator and a glucocorticoid, oxygen supplementation, minimal handling/restraint, and sedation as needed. Stable asthmatic cases should receive lifelong glucocorticoids, plus bronchodilators if necessary, but environmental modification and weight management strategies are mandatory for all affected animals. Therapy should be individualized to each cat, with tapering of medications ideally focused on resolution of both clinical signs and airway inflammation when possible.
Padrid P. Chronic bronchitis and asthma in cats. In: Bonagura J, Twedt D (eds.) Current Veterinary Therapy XIV. Philadelphia: WB Saunders; 2009;650-658.
Reinero CR. Advances in the understanding of pathogenesis, and diagnostics and therapeutics for feline allergic asthma. Vet. J. 2011;190:28-33.
Nafe LA, DeClue AE, Lee-Fowler TM, et al. Evaluation of biomarkers in bronchoalveolar lavage fluid for discrimination between asthma and chronic bronchitis in cats. Am. J. Vet. Res. 2010;71:583-591.
Reinero CR, Masseau I, Grobman M, et al. Perspectives in veterinary medicine: description and classification of bronchiolar disorders in cats. J. Vet. Intern. Med. 2019;33:1201-1221.
Adamama-Moraitou KK, Patsikas MN, Koutinas AF. Feline lower airway disease: a retrospective study of 22 naturally occurring cases from Greece. J. Feline Med. Surg. 2004;6(4);227-233.
Lisciandro GR. Abdominal and thoracic focused assessment with sonography for trauma, triage, and monitoring in small animals. J. Vet. Emerg. Crit. Care (San Antonio). 2011;21:104-122.
Trzil JE. Feline Asthma: Diagnostic and Treatment Update. Vet. Clin. North Am. Small Anim. Pract. 2020;50:375-391.
Masseau I, Reinero CR. Thoracic computed tomographic interpretation for clinicians to aid in the diagnosis of dogs and cats with respiratory disease. Vet. J. 2019;253:105388.
van Eeden ME, Vientós-Plotts AI, Cohn LA, et al. Serum allergen-specific IgE reactivity: is there an association with clinical severity and airway eosinophilia in asthmatic cats? J. Feline Med. Surg. 2020;22:1129-1136.
Reinero CR, Delgado C, Spinka C, et al. Enantiomer-specific effects of albuterol on airway inflammation in healthy and asthmatic cats. Int. Arch. Allergy Immunol. 2009;150:43-50.
Cocayne CG, Reinero CR, DeClue AE. Subclinical airway inflammation despite high-dose oral corticosteroid therapy in cats with lower airway disease. J. Feline Med. Surg. 2011;13:558-563.
Carol Reinero
Dr. Reinero graduated from the University of California, Davis in 1995 before completing a small animal internal medicine residency and a PhD in Immunology at the same institution Read more
Lungworm and heartworm are an underestimated but potentially serious threat for many cats, as this article reveals.
Diaphragmatic hernia is a common consequence of traumatic injury in cats and may be fatal if not promptly diagnosed and treated; this article reviews the pathophysiology and treatment of the condition.
Chylothorax is a differential for any cat with pleural effusion; here Elizabeth Rozanski describes her preferred approach to such cases.
Lymphoma is one of the most common neoplasms of cats, and the mediastinal form can be a major differential for a cat that presents with respiratory signs, as James Elliott describes.